The science of human connection

What relationships do to the body and mind — and why they may be the most underrated determinant of health-span
Key takeaways
• Social connection meets Bradford Hill criteria for a causal — not merely associative — link with health and mortality.
• Loneliness and isolation elevate mortality risk comparably to smoking 15 cigarettes a day, exceeding physical inactivity and obesity.
• Mechanisms are biological: stress-axis dysregulation, elevated inflammation, disrupted sleep, and immune suppression.
• Quality of social ties predicts health outcomes more reliably than quantity; conflict-heavy relationships can be actively harmful.
• Social connection shapes health behaviours across the life course — dietary choices, physical activity, sleep, and healthcare engagement.
• Even modest improvements in social connection produce measurable changes in physical and mental health markers.
The claim that human connection is good for us sounds self-evident. Of course relationships matter. Of course loneliness is unpleasant. These feel like truisms rather than scientific findings.
But what the research actually shows goes considerably further than popular wisdom suggests — and considerably further than most health communication conveys. Social connection does not merely make life more enjoyable. It is a measurable biological determinant of physical health, mental health, cognitive function, and longevity. Its absence causes harm through mechanisms that are now reasonably well understood. And its importance across the life course rivals — and in some contexts exceeds — diet, physical activity, and other behaviours we treat as obvious health priorities.
This companion piece sets out what the evidence actually shows, how researchers study it, what the biological mechanisms are, and what it means in practical terms for how we think about the role of relationships in a healthy life.
How researchers study social connection and health
The study of social relationships and health faces methodological challenges similar to those in nutrition research: people cannot be randomised to social conditions across decades, self-reported data is imprecise, and confounding variables are numerous. The field uses several complementary approaches:
• Epidemiological cohort studies — large populations followed over years or decades, with social measures (network size, perceived support, loneliness, marital status) tracked alongside health outcomes. These generate the majority of the observational evidence.
• Meta-analyses and systematic reviews — pooling data across many studies to identify consistent signals across populations, cultures, and measurement approaches. The most cited findings in this field come from meta-analyses covering millions of participants.
• Mechanistic and biomarker studies — examining how social conditions affect measurable biological parameters: cortisol, inflammatory markers such as IL-6 and CRP, cardiovascular function, immune activity, sleep architecture, and gene expression.
• Randomised trials of social interventions — testing whether structured programmes to increase social connection produce measurable health improvements. These are harder to run than drug trials but increasingly common.
The case for social connection as a health determinant does not rest on any single study. It rests on convergence: observational data, mechanistic research, and intervention evidence all pointing in the same direction across different populations and measurement methods. A 2019 analysis in SSM — Population Health argued that this body of evidence now satisfies the Bradford Hill criteria for establishing causation — the same framework used to establish the causal link between smoking and lung cancer.
KEY RESEARCH
Howick, J., Kelly, P., & Kelly, M. (2019). Establishing a causal link between social relationships and health using the Bradford Hill Guidelines. SSM — Population Health, 8. https://doi.org/10.1016/j.ssmph.2019.100402
The mortality finding — and why it is serious
The most striking finding in this literature — and the one most frequently cited in public health discussions — concerns the relationship between social connection and survival.
A meta-analysis by Holt-Lunstad and colleagues, drawing on data from 308,849 participants across 148 studies, found that individuals with adequate social relationships had a 50% greater likelihood of survivalover a given follow-up period compared to those with poor or insufficient social connection. When the researchers compared social isolation's effect on mortality risk to other established risk factors, it exceeded the risk associated with physical inactivity, obesity, and excessive alcohol consumption — and was comparable to smoking 15 cigarettes a day.
People with adequate social relationships have a 50% greater likelihood of survival than those with poor social connection — a risk comparable to smoking 15 cigarettes a day.
These are not marginal effects. A 2021 review in Current Directions in Psychological Science summarised the evidence across multiple meta-analyses and concluded that social connection is a major health implication that warrants inclusion alongside diet and physical activity as a core public health priority.
A 2016 study in the Proceedings of the National Academy of Sciences followed participants across the life course and found that social isolation was associated with elevated inflammation in adolescence — comparable in effect to physical inactivity — and with hypertension risk in old age that exceeded the risk attributable to clinical diabetes. The effects are not confined to later life: they accumulate across decades.
KEY RESEARCH
Yang, Y., Boen, C., Gerken, K., Li, T., Schorpp, K., & Harris, K. (2016). Social relationships and physiological determinants of longevity across the human life span. Proceedings of the National Academy of Sciences, 113, 578–583. https://doi.org/10.1073/pnas.1511085112
Biological mechanisms — how connection (and isolation) affect the body
The question of how social relationships translate into physical health outcomes has been increasingly well answered by mechanistic research. Several pathways are now well-characterised.
The stress axis and cortisol
Chronic social isolation keeps the hypothalamic-pituitary-adrenal (HPA) axis — the body's primary stress-response system — in a state of elevated activity. Cortisol levels remain higher for longer in people who feel chronically lonely or unsupported. Sustained cortisol elevation has downstream effects on immune function, cardiovascular health, metabolic regulation, and sleep quality.
Social support acts as a stress buffer: the presence of trusted others dampens HPA-axis reactivity in the face of acute stressors, reducing the magnitude and duration of cortisol responses. This buffering effect is one of the best-replicated findings in social psychophysiology.
Inflammation
Loneliness and social isolation are consistently associated with elevated markers of systemic inflammation — including interleukin-6 (IL-6) and C-reactive protein (CRP). Chronic low-grade inflammation is a contributor to cardiovascular disease, type 2 diabetes, certain cancers, and neurodegenerative conditions. The association between social isolation and elevated inflammation has been replicated across age groups and populations, with effect sizes that are clinically meaningful.
Conversely, positive social relationships are associated with lower inflammatory burden, possibly through stress-buffering mechanisms and through the behavioural pathways described below.
Cardiovascular function
Social isolation and loneliness are associated with elevated blood pressure, reduced heart rate variability, and higher risk of cardiovascular events including heart attack and stroke. A 2024 systematic review in Healthcare found consistent evidence linking social isolation to adverse cardiovascular outcomes across a range of study designs and populations. The mechanisms likely include both the direct effects of chronic stress-axis activation and the indirect effects of isolation on health behaviours.
Immune function and infection risk
Research has found that social isolation is associated with poorer immune responses — including reduced vaccine efficacy and greater susceptibility to viral infection. Loneliness has been shown to predict faster progression of illness and slower recovery. The COVID-19 pandemic provided a natural experiment in extreme social restriction, with emerging evidence suggesting that the health effects of isolation extended well beyond the direct effects of the virus.
Sleep
Loneliness and social isolation are associated with disrupted sleep — more fragmented, less restorative, and associated with greater fatigue despite equivalent hours. The relationship appears bidirectional: poor social connection disrupts sleep, and poor sleep further impairs social functioning and mood. Given the centrality of sleep to virtually every other health system, this pathway alone has substantial downstream significance.
KEY RESEARCH
Holt-Lunstad, J. (2024). Social connection as a critical factor for mental and physical health: evidence, trends, challenges, and future implications. World Psychiatry, 23. https://doi.org/10.1002/wps.21224
Mental health: what the evidence actually shows
The relationship between social connection and mental health is among the most consistently replicated in the behavioural sciences. The 2022 scoping review by Wickramaratne and colleagues — covering 80 studies and over 2 million participants — concluded that social connectedness is a significant determinant of mental health across the life course, with effects observed for depression, anxiety, loneliness, psychological well-being, and social functioning.
KEY RESEARCH
Wickramaratne, P., Yangchen, T., Lepow, L., Patra, B., Glicksburg, B., Talati, A., et al. (2022). Social connectedness as a determinant of mental health: A scoping review. PLoS ONE, 17. https://doi.org/10.1371/journal.pone.0275004
Depression and anxiety
Longitudinal studies consistently find that low perceived social support and high loneliness at baseline predict later depression and anxiety — not merely concurrent association. The effect sizes are substantial. A 2021 umbrella review in BMJ Open, examining meta-analyses of the physical distancing literature, concluded that reduced social connection is a risk factor for both incident and persistent mental health problems, with the relationship likely bidirectional: mental illness can also reduce social connection, creating feedback loops that sustain both.
Resilience and recovery
Social ties do not only prevent mental health problems; they support recovery from them. People with stronger social support networks have better outcomes following depression, trauma, bereavement, and serious illness. Support functions through multiple channels: practical assistance, emotional validation, access to information and healthcare, and the maintenance of routine and purpose — all of which are destabilised by social isolation.
Later life
The mental health benefits of social connection are particularly well-documented in older adults. Research by Rook and Charles (2017) found that close social ties in later life are independently associated with better psychological health, even controlling for physical health status. Positive relationships with others are associated with a sense of purpose, reduced existential anxiety, and better emotional regulation. Importantly, this research also highlights the cost of low-quality relationships: high-strain social ties are associated with worse psychological outcomes than having fewer but higher-quality connections.
Social connection and health behaviours
Beyond its direct biological effects, social connection influences health through the behavioural pathways it shapes. A 2023 paper in Lifestyle Medicine by Proctor, Barth, and Holt-Lunstad framed the relationship explicitly: a healthy lifestyle is, in substantial part, a social lifestyle.
KEY RESEARCH
Proctor, A., Barth, A., & Holt-Lunstad, J. (2023). A healthy lifestyle is a social lifestyle: The vital link between social connection and health outcomes. Lifestyle Medicine. https://doi.org/10.1002/lim2.91
The mechanisms here are multiple and interactive:
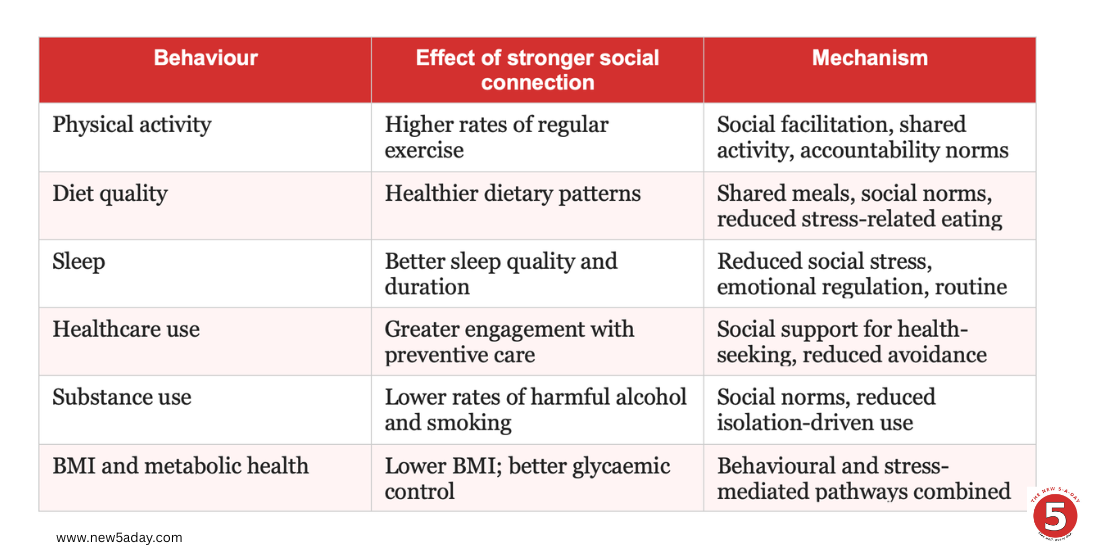
These behavioural effects compound over time. A person embedded in a social network that values physical activity, regular meals, and reasonable sleep is, by the ordinary mechanisms of social influence, more likely to sustain those behaviours. The converse is equally true: social isolation tends to be associated with the gradual erosion of health-supporting routines.
Quality versus quantity — a critical distinction
One of the most clinically important nuances in this literature is the distinction between the size of a social network and the quality of the relationships within it.
A large body of evidence — including Holt-Lunstad's meta-analyses, longitudinal work by Umberson and Montez (2010), and more recent studies focused on relationship quality in later life — consistently finds that it is perceived social support, emotional closeness, and relationship quality that predict health outcomes, rather than network size or frequency of contact alone.
High-conflict or high-strain relationships can be actively harmful. Research by Rook and Charles (2017) found that negative or demanding social ties were associated with worse health outcomes than low social contact — suggesting that not all connection is beneficial, and that the presence of people is not the same as the presence of support.
A 2023 paper by Friedman and colleagues, examining data from a large cohort of older adults, found that positive relations with others — a measure of relationship quality, not quantity — independently predicted fewer functional limitations and lower all-cause mortality, even after controlling for network size, perceived support, and a range of health covariates.
KEY RESEARCH
Friedman, E., Franks, M., Teas, E., & Thomas, P. (2023). Social connectedness, functional capacity, and longevity: A focus on positive relations with others. Social Science & Medicine, 340, 116419. https://doi.org/10.1016/j.socscimed.2023.116419
The practical implication is clear: the goal is not to maximise social contact but to cultivate relationships that are genuinely supportive, reciprocal, and characterised by positive regard. A few such relationships are worth far more than a large network of superficial or conflicted ties.
Cognitive health and ageing
The relationship between social connection and cognitive health is an increasingly important area of research, particularly given demographic trends in ageing populations.
Social engagement appears to support cognitive reserve — the brain's capacity to sustain function in the face of age-related change — through several overlapping mechanisms: the cognitive demands of conversation and relationship maintenance, the emotional regulation that social support facilitates, and the reduction of chronic stress that would otherwise accelerate neurobiological ageing.
Longitudinal studies consistently associate greater social engagement with slower rates of cognitive decline and lower dementia risk. A scoping review by Lem and colleagues (2021) in BMC Geriatrics found that, among long-term care residents, greater social connection was associated with better cognitive and physical health outcomes and reduced mortality — a finding that held across different measures of social engagement and different outcome assessments.
The cognitive benefits of social engagement are relevant across the life course, not only in old age. Regular social interaction in midlife appears to be protective, and the social networks established earlier in life create a resource that can be drawn on during the cognitive challenges of later decades.
Social connection across the life course
The health effects of social connection are not confined to any particular life stage. Evidence suggests they operate — and that the costs of isolation accrue — from childhood through old age.
Early life and adolescence
The quality of early social attachment shapes biological stress-response systems in ways that have long-term consequences. Adverse early social experiences — neglect, isolation, chronic conflict — are associated with dysregulation of the HPA axis that persists into adulthood. The Yang et al. (2016) PNAS study found that low social connection in adolescence predicted elevated inflammatory markers — an effect comparable in magnitude to that of physical inactivity.
Midlife
Social networks typically peak in early adulthood and begin to contract through midlife as work, family, and geographic mobility reshape the social landscape. This contraction — often experienced as a gradual drift rather than a deliberate choice — is associated with declining social support at a life stage when occupational stress and health demands are often high. Intentional maintenance of social connection in midlife is associated with better health outcomes in later decades.
Later life
Older adults face particular social risks: bereavement, retirement, physical mobility constraints, and the gradual loss of contemporaries can reduce social networks substantially. Lem and colleagues (2021) and Lim and colleagues (2023) both found that social connection in long-term care settings was associated with better quality of life, better health outcomes, and delayed mortality — suggesting that social engagement retains its health significance even in contexts of high physical dependency.
The loneliness epidemic — understanding the context
The public health framing of loneliness as an epidemic is not rhetorical excess. Evidence across multiple countries suggests that a significant and growing proportion of the population experiences chronic loneliness or social isolation. UK data indicate that loneliness is particularly prevalent among young adults, older adults, people with disabilities or chronic illness, and those who have experienced significant life transitions.
The structural causes are well-documented: declining participation in civic and community institutions, increasing residential mobility, changes in work patterns (including remote work), reduced intergenerational contact, and the partial displacement of in-person social interaction by digital communication. None of these causes is inherently problematic, but their combined effect has been a reduction in the incidental social contact and embedded community life that historically supported connection without requiring active effort.
Technology merits particular attention. Digital communication extends the reach of social connection and can maintain relationships across distance. But it does not fully replicate the health effects of in-person contact: the physiological co-regulation that occurs in physical proximity — affecting heart rate, breathing, cortisol, and oxytocin — is largely absent from screen-mediated interaction. The relationship between social media use and loneliness is complex and contested in the literature, but there is reasonable evidence that passive consumption of social media can increase loneliness rather than reducing it.
Social connection and the other pillars
From the perspective of The New 5-a-Day framework, social connection does not operate in isolation from the other four pillars — it is woven through all of them.
• Sleep Well: Loneliness disrupts sleep architecture. Social conflict is among the most common causes of hyperarousal at bedtime. Positive social relationships, by contrast, support emotional regulation and reduce the rumination that underlies insomnia.
• Eat Well: Social eating is consistently associated with better dietary quality and greater meal satisfaction. Social isolation is associated with irregular eating patterns, reduced dietary variety, and greater reliance on convenience foods.
• Be Active: Physical activity is more likely to be initiated and sustained when it is social. Group exercise, team sport, walking with others, and activity built around social connection show higher adherence rates than solitary exercise for most people.
• Me-Time: The restorative value of solitude is greater when it is freely chosen against a backdrop of adequate social connection. Isolation and solitude are not the same thing: chosen aloneness is restorative; unwanted aloneness is harmful.
This interconnection is not incidental. The pillars of The New 5-a-Day are interdependent because health itself is interdependent: the systems that regulate sleep, metabolism, movement, emotional well-being, and social function are not separate. They are aspects of a single integrated organism, shaped by a lifetime of behaviour and relationship.
Putting it together: connection as a determinant of health-span
The evidence on social connection and health-span converges on conclusions that are both scientifically robust and practically significant:
• Social connection meets the criteria for a causal — not merely associative — influence on physical health, mental health, and mortality.
• The biological mechanisms are multiple and well-characterised: stress-axis regulation, inflammation, cardiovascular function, immune activity, and sleep are all influenced by the quality of social ties.
• The health consequences of social isolation are comparable in magnitude to those of established risk factors such as smoking and physical inactivity — yet receive far less attention in public health communication.
• Quality of social connection matters more than quantity: a small number of genuinely supportive relationships confers substantially greater health benefit than a large network of superficial or conflicted ties.
• Social connection shapes health behaviours — diet, activity, sleep, healthcare engagement — as well as biological parameters directly, making it a foundational influence on the conditions that determine health-span.
• The effects operate across the entire life course, from early developmental biology through to the determinants of healthy ageing.
As Pillar Five of The New 5-a-Day, Find Your People sits at the intersection of biology, behaviour, and meaning. Connection is not separate from health — it is one of its most powerful determinants. The science supports investing in it with the same seriousness we give to diet and exercise: intentionally, consistently, and with an understanding of what is actually at stake.
A note on medical advice: The content in this post is intended to inform and inspire, not to replace professional medical guidance. If anything you've read raises questions or concerns about your own health, please speak to your GP or another qualified health professional.
[Read the Open Post →] [View the References →] [Listen to the Episode →]